

Do Viruses Really Transmit Between Mammals?
A critical review of James Hill’s 12 cited studies using the Transmission Credibility Metric

Transmission Credibility Metric (TCM) - To use the TCM, one can simply upload any transmission paper together with the prompt and include the instruction: “Use the attached prompt to evaluate the attached paper.”
Introduction: Findings from My Paper
In my paper, Reevaluating Viral Transmission: A Critical Examination of Virological Methods and Assumptions, I analyzed over 150 studies that claimed to demonstrate viral transmission. My conclusion was stark: these studies consistently fail to establish credible, natural host-to-host contagion. Instead, they rely on artificial inoculations, proxies like PCR and serology, and procedures that themselves may cause symptoms.
This work shows that what is widely accepted as “proof” of viral transmission is, in fact, deeply flawed.
The Transmission Credibility Metric (TCM)
To make these evaluations systematic and transparent, I developed the Transmission Credibility Metric (TCM).
This structured prompt guides readers through nine core reasons to doubt transmission experiments, as well as a set of extended considerations. The TCM is designed to be reproducible — anyone can use it to assess transmission studies for themselves.
The framework emerged from the research process behind my paper, where recurring methodological flaws were distilled into a clear and practical tool. To use the TCM, one can simply upload any transmission paper together with the prompt and include the instruction: “Use the attached prompt to evaluate the attached paper.”
The prompt is also presented below and can be copied for use elsewhere (or improved upon):
Prompt for Evaluating Transmission Studies – rv0 Sept 2025 (Matthew North)
You are an expert reviewer of virology transmission studies. Your task is to critically evaluate whether a study provides sound evidence of natural transmission. Follow the steps below.
Summarize the study’s design, methods, and findings. The findings must be very detailed on the symptoms documented (e.g. runny nose, fever, etc which could be as a result of the study method itself).
Evaluate against the below considerations and give the result in table format (columns: Reason number, Reason, Accounted for?, Notes).
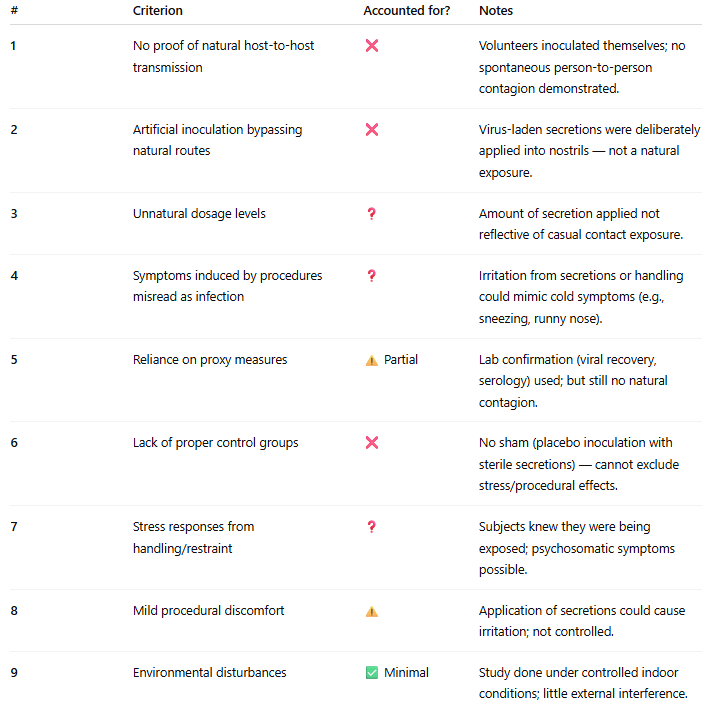
Evaluate against the core 9 reasons to doubt transmission experiments. For each reason, state whether the study accounts for it, fails to account for it, or leaves it unclear, and give short notes:
No proof of natural host-to-host transmission
Artificial inoculation bypassing natural routes
Unnatural dosage levels
Symptoms induced by procedures misread as infection
Reliance on proxy measures instead of direct evidence
Lack of proper control groups
Stress responses from handling or restraint
Mild procedural discomfort
Environmental disturbances during monitoring
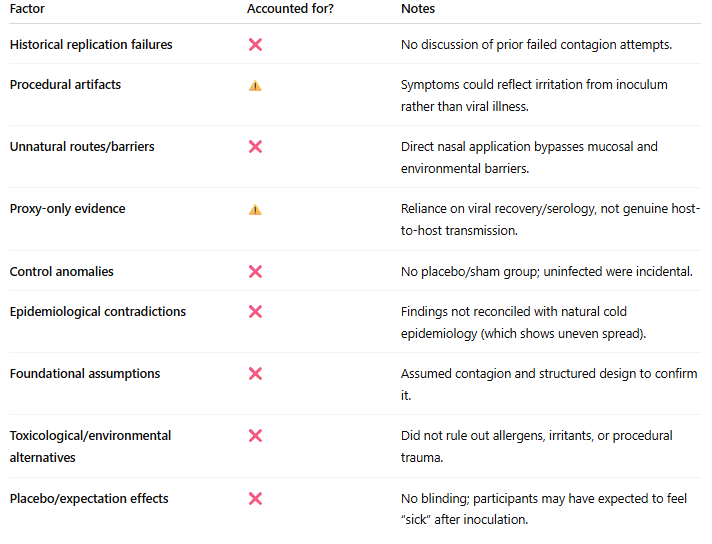
Evaluate against extended considerations. These address deeper historical and methodological concerns:
Historical replication failures — has natural transmission ever been reliably demonstrated in controlled settings across history?
Procedural artifacts — could symptoms have been caused by the procedures themselves (e.g., inoculation trauma, swabbing, blood draws, intubation)?
Unnatural routes and barriers — does the method bypass natural defenses such as the blood–brain barrier, gastric acid, or intact mucosa?
Proxy-only evidence — does the study rely solely on PCR positivity, cytopathic effect, or other indirect measures without showing illness through natural exposure?
Control anomalies — do placebo or sham groups sometimes show equal or greater illness than exposure groups?
Epidemiological contradictions — do real-world patterns (family spread, hospital clusters, rural vs. urban prevalence, abrupt epidemic cessation) align with the claimed transmission route?
Foundational assumptions — does the study presuppose contagion or infection without demonstrating it?
Toxicological and environmental alternatives — were chemical, nutritional, or environmental causes considered and ruled out?
Placebo and expectation effects — could illness be triggered by belief in exposure, stress, or psychosomatic mechanisms?
Further Instructions:
Highlight the issues that most seriously undermine the study’s validity
Conclude with a judgment: does the study provide credible evidence of natural transmission, or is it undermined by methodological flaws?
Give a final score out of 10, where 10 = exceptionally well-constructed and executed, and 0 = very poorly constructed and executed. Call the results from this prompt the Transmission Credibility Metric.
Example: Evaluating One Study
Study Title: Transmission of rhinovirus colds by self-inoculation
Citation: Gwaltney JM Jr, Hendley JO, Wenzel RP. New England Journal of Medicine. 1973;288(26):1361–1364.
1. Study Summary
Objective: To determine whether self-inoculation of nasal secretions could transmit rhinovirus colds in volunteers.
Subjects: Human adult volunteers (medical students and staff).
Design:
Donors: Infected volunteers produced nasal secretions containing rhinovirus.
Recipients: Healthy subjects applied these secretions to their own nasal mucosa (self-inoculation).
Controls: A “hand contact only” group touched contaminated surfaces or hands but did not self-inoculate.
Outcomes:
Symptoms recorded (nasal discharge, congestion, sore throat, cough).
Viral recovery from nasal washings and serology to confirm infection.
Results:
High attack rate in self-inoculated subjects (~65%).
Very low infection rate in contact-only group.
Authors concluded that self-inoculation of secretions to nasal mucosa is an efficient mode of rhinovirus transmission.
2. Core 9 Reasons to Doubt Transmission Experiments
3. Extended Considerations
4. Key Undermining Issues
No natural contagion tested — outcome was forced self-inoculation.
Artificial exposure route — bypassed normal transmission pathways.
No placebo control — impossible to separate genuine infection from irritation or expectation.
Symptoms mild and nonspecific — easily explained by procedures or psychosomatic effects.
5. Judgment
This study demonstrated that if you directly place rhinovirus secretions into your own nose, you may develop a cold. That is not evidence of natural viral transmission between humans.
The methodology is artificial, control conditions are weak, and outcomes rely on proxies and subjective symptom reports.
Transmission Credibility Metric Score: 3/10
Strengths: Clear methods, viral confirmation.
Weaknesses: No natural host-to-host spread, no sham controls, artificial procedures, non-specific outcomes.
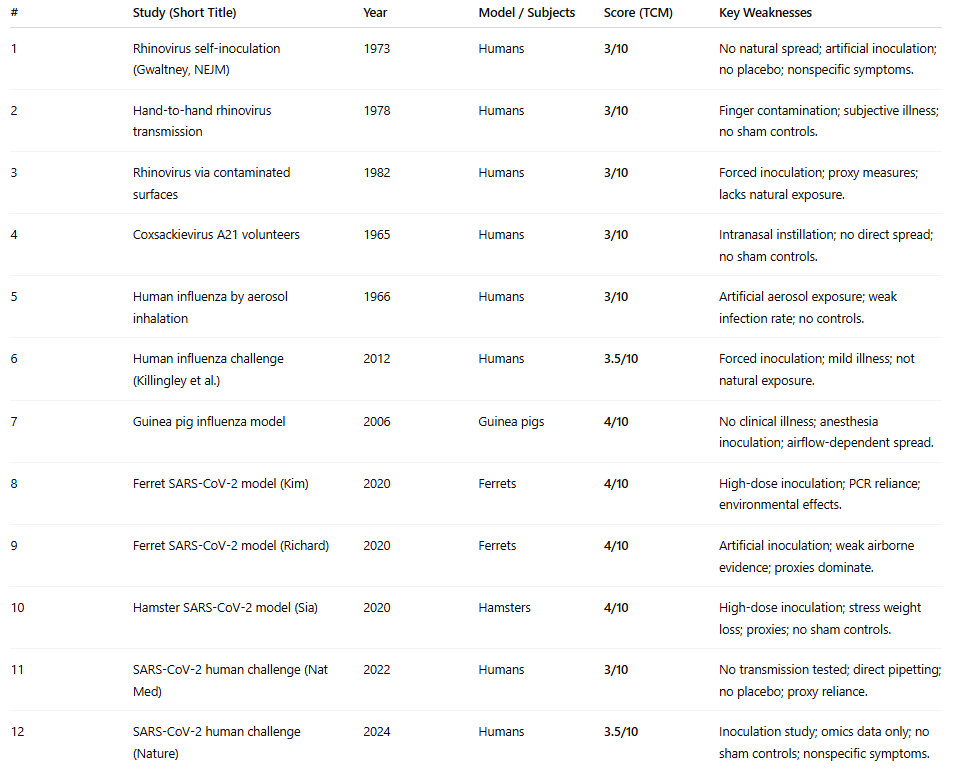
Results Across All 12 Studies
Using the TCM, I assessed all 12 studies that James Hill presented in his Substack post “Yes, viruses transmit between mammals.”
Here are the results:
Conclusion
The twelve studies highlighted by James Hill are weak examples of transmission research, several of which I have already evaluated in detail in my paper. None provide credible evidence of natural host-to-host spread. Instead, they exemplify the methodological flaws documented across more than 150 studies—artificial inoculation, reliance on indirect proxies, inadequate controls, and a consistent failure to account for external factors such as stress, environment, and procedure-induced symptoms.
Taken together, these findings reveal that the supposed “proof” of viral contagion rests on fragile and unconvincing foundations. The Transmission Credibility Metric makes this plain: not one of these highly cited studies scores above 4/10. In fact, I would argue that even a score of 4/10 is overly generous unless natural transmission can first be demonstrated under conditions free of such methodological shortcomings.
Thank you for this. I generally respect Dr. Hill but he has totally lost the plot with his absurd attachment to believing in contagious "viruses" that even jump species! How ridiculous it is.
Excellent work, I will use that prompt in the future, I just finished looking at the first study before stumbling upon your post expecting to debunk all of the other studies he cited, but looks like you already exposed their flaws enough. Anyway, here is my critique of the first study as well:
"Transmission of rhinovirus colds by self-inoculation" -The researches watched some people picking their nose, using their pseudo-scientific method of cell cultures, they "measured" how often the "virus" spread/stayed on different materials/people's skin/body parts, how often it was present in the coughs, sneezes, throats, noses, saliva and hands.
They got volunteers to touch their cell culture fluid with their finger and then rub their eyes/stick up their noses.
They then swabbed their throat/nose a couple times and tested for CPE/antibodies, they also monitored for 8 non specific "symptoms" (sneezing, nasal discharge, nasal obstruction, sore/dry/itchy throat, cough, headache, malaise, and chilliness) to occur over the next 6 days scored on severity of 1-4 requiring only a score of 5 in TOTAL plus either 3 days of runny nose and/or the volunteers opinion that they have a cold like illness. Yet only 4/11 volunteers met this weak ass criteria.
No placebo/blinding/control group, no independent variable, no actual dependent variable, indirect pseudoscientific measurements throughout.